Legacy Devices are the medical devices covered by a valid Directive certificate under Directive 93/42/EEC or Directive 90/385/EEC and continue to be placed on the market after the date of application of Regulation (EU) 2017/745 (MDR).
Those devices should be registered under EUDAMED without Basic UDI-DI and a UDI-DI within 18 months after the application is placed or 24 months if the EUDAMED is not fully functional before the date of application.
This registration is mandatory for the manufacturer in case of any serious incidents and if any field safety actions have been taken, at least before the final vigilance report is submitted.
As per MDR device requirements, any medical device registered under EUDAMED will require Basic UDI-DI and UDI-DI, which gets reflected on the database design for future reference.
These legacy devices will need two other unique access keys (UI) to replace basic UDI-DI and UDI-DI to register under EUDAMED. Instead of Basic UDI-DI, the legacy devices will be assigned EUDAMED DI, and instead of UDI-DI, the legacy devices will be assigned EUDAMED ID.
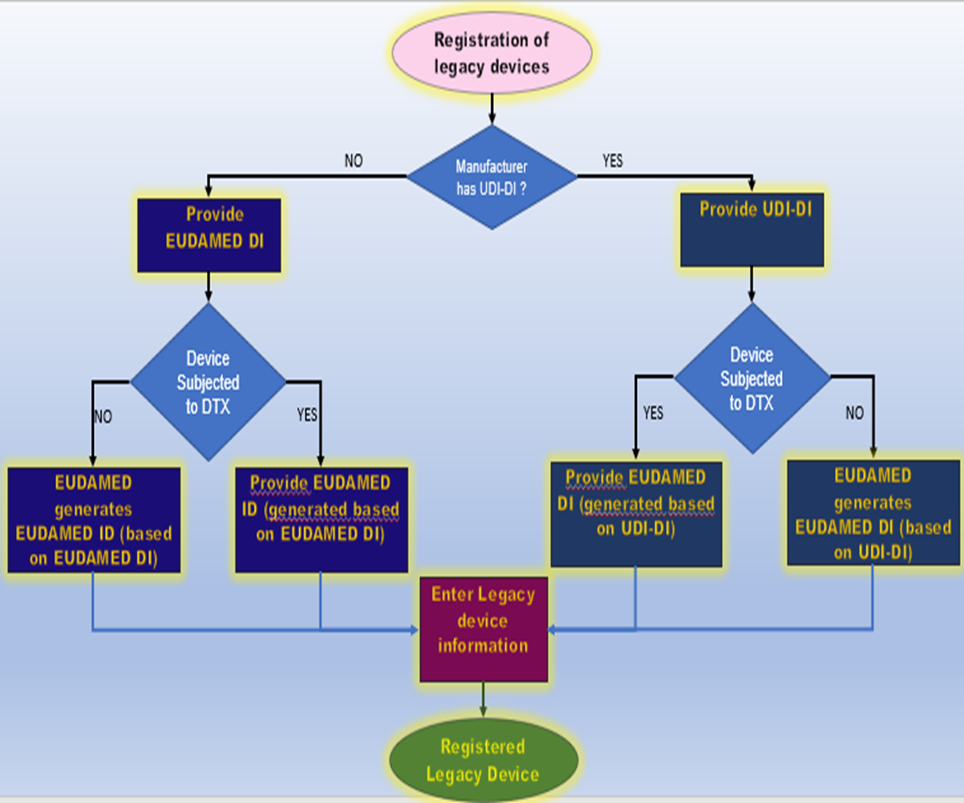
Registration of Legacy Devices
As per the flowchart above,
If the manufacturer already has UDI-DI assigned to the legacy device, then the EUDAMED DI will be automatically generated based on UDI-DI in the standard format, placing the character “B-“ in front of UDI-DI
If the manufacturer does not have an assigned UDI-DI for the legacy device, then they will be assigned both EUDAMED DI and EUDAMED ID
The EUDAMED DI can be completely assigned by the EUDAMED or partially taken from the manufacturer using their DI code. But the EUDAMED ID should be completely generated by the EUDAMED.
The EUDAMED DI will start with the character “B”, whereas the EUDAMED ID will start with the character “D” other than the first character EUDAMED DI and the ID will include the SRN number, a number assigned to the manufacturer and check digit.
In addition, the manufacturer should enter their directive certificate identification, such as NB number, revision number, certificate number, and expiry date.
EUDAMED allows the linking of the regulation device with the legacy devices, if the regulation device is exactly the same as the legacy device, they can have the same UDI-DI.
This link may happen automatically by EUDAMED, or the manufacturer can create a link manually by assigning a legacy device identifier, which should happen at the level of UDI-DI.
FAQ
What is the difference between Basic UDI-DI and a UDI-DI?
Basic UDI-DI is a DI assigned to the level of unit use of the device, which is a primary identifier for the device model/family . It is mentioned in the reference CE certificates and the Declaration of Conformity. In contrast, UDI-DI is a unique numeric or alphanumeric code of each device itself , which is used as an access key for the UDI database.
What is EUDAMED?
EUDAMED is a European Database of Medical devices operated by the European Commission to register relevant information on medical devices and to ensure the medical devices’ safety, traceability, and transparency as per MDR 2017/745.
When can a manufacturer register under EUDAMED?
The manufacturer can register their device information/UDI voluntarily in EUDAMED. Moreover, it is mandatory to register legacy and regulatory devices within 24 months after the Commission publishes that the EUDAMED is completely functional.
The Medical Device Vigilance System’s goal is to lower the risks of using medical equipment and serious incidents while it strives to improve protection for patients, healthcare providers, and other users.
A National Competent Authority Report is one way that adverse occurrences are evaluated and, where necessary, information is shared according to the Medical Devices Directives/Regulations (NCAR).
The implementation of suitable field safety corrective measures aims to prevent the repetition of such events. To facilitate and harmonise the execution of the EU regulations on Medical Devices by manufacturers and competent authorities, general recommendations on vigilance are added to the Medical Devices Regulations.
Manufacturers of medical devices are obligated by law to report adverse incidents and Field Safety Corrective Actions (FSCAs) to EU Competent Authorities in accordance with the European Medical Devices Regulations and the In-Vitro Diagnostic Devices Regulations.
Regulators are frequently perplexed by the “when, what, and to whom” part of EU incident reporting. Companies that disclose incidents incorrectly risk serious repercussions. RA professionals must take the initiative because ignorance is not a valid justification for failing to report problems.
Requirements for Vigilance Reporting According to EU MDR 2017/745
The following events are considered as “reportable events” in accordance with the new EU MDR when they directly involve a medical device:
The event resulted in death or a severe decline of the health of the patient, user, or any other person involved.
Although the specific event had no adverse effects on any individual, it could result in death or a severe decline of the health of the patient, user, or any other individual if it were to occur again. The manufacturer is responsible for determining whether a given occurrence could seriously impact a patient or user; this assessment must be based on risk management and a medical examination of the particular event.
The Timeline For Vigilance Reporting (as per MDR ARTICLE 87)
Events that pose a serious risk to public health must be notified immediately but no later than two days after becoming aware of them.
Events involving the death of a patient, a user, or any other person, or the serious deterioration of their health, must be notified immediately but no later than 10 days after becoming aware of them.
Events that had little or no impact on the patient or user but were likely to result in death or a major decline in health if they happened again must be reported right away but no later than 15 days after becoming aware of them.
When are EU vigilance reports necessary?
In accordance with MEDDEV 2.12/1, an incident report must be made if a device malfunction, decline in device performance, inadequate instructions, or inadequate labelling results in death or serious injury, or if it could result in death or serious deterioration of state of health if it were to occur again.
The incident has to be notified to the member state’s Competent Authority (CA), depending on where it happened.
In Europe, below are the fundamental procedures to report an incident:
The appropriate reporting deadline, which will depend on the severity of the incident, can be found in MEDDEV 2.12/1.
Notify the relevant Competent Authorities of the incident.
Respond to Competent Authorities’ inquiries on the devices implicated, their time on the market, and any design alterations.
Appropriate communication with the Competent Authorities and determine whether a Field Safety Corrective Action (FSCA) and Field Safety Notice (FSN) are required.
Send a Final Incident Report or a FSCA Report to the appropriate authorities.
Include vigilance reports in ISO 13485 or equivalent quality system records and any correspondence with Competent Authorities.
Unless Class 1 self-certified, report any accidents or FSCAs to the respective Notified Body.
Vigilance as per EU MDR compared to the MDD
It was challenging to distinguish between Vigilance and PMS in the Medical Device Directive (MDD).
In the European Union Medical Device Regulation (EU MDR), a distinction is made between “post-market surveillance” (PMS), which is the periodic reconfirmation that the benefits of the device continue to outweigh its risks, and “vigilance,” which is the identification, reporting, and trending of serious incidents and the conduct of safety-related corrective actions.
The 10-day limit for reporting a death or a major health deterioration and the 2-day reporting deadline for serious threats to the public’s health have not changed since the MDD.
The MDD’s 30-day reporting deadline for all other reportable occurrences is replaced by a 15-day reporting deadline for all other major incidents.
When the frequency or seriousness of additional incidents significantly increases, the EU MDR also mandates vigilance reporting. As opposed to the MDD, trend reporting (Article 88) and analysis (Article 89) were already directed by MEDDEV 2.12/1 and had been anticipated by European Competent Authorities and Notified Bodies for some time.
The necessity to submit vigilance reports to the EUDAMED database (Article 92), as opposed to each national Competent Authority, as required under the MDD, is a new requirement in the EU MDR.
The national vigilance reporting methods will continue to be used, though, until the vigilance module of EUDAMED is available.
FAQs
To Whom Should Medical Device-Related Incidents Be Reported?
Medical device-related adverse events must be reported to the relevant national competent authorities where they occurred.
A short article based on MDCG 2021-22 guidelines on “first certification for the type of devices and the corresponding procedures to be followed by the Notified Bodies, ” established based on Article 106 of Regulation 2017/745 for Class D IVDR devices.
Additionally, this guide talks about the conditions to be followed by the Notified bodies, whether to consult the expert panel for the performance evaluation report of the IVDR devices.
If the type of the device comes under the first certification in the market (AND)
There is no CS for the class D devices.
According to Article 48(6) of IVDR 2017/746, the first certification for the type of device means that the product has no similar product with the same intended use or technology around the European market.
Also, the notified bodies should submit the performance evaluation report to the expert panel within five days of receiving it from the manufacturer. The same intended purposes include
Device functions like monitoring, diagnosing, screening etc.
If the device is quantitative, semi-quantitative or qualitative
It is automated or semi-automated, or not
If it is used for any measurement
If the device is used for any specific disorder
What is the specimen type, or if it is applicable for some testing purpose
What all the intended users
Or if the device has the same principle of operation
Suppose the IVDR devices has met the above-mentioned purposes under Directive 98/79/EC or has an ongoing consultation with the expert panel under EU 2017/746. In such case, the notified bodies need not consult the expert panel for the certification.
However, if the class D device is with similar intended purpose but one of the IVDR devices has some additional intended purpose along with the common intended purpose, which falls outside Rule 1 or 2 of IVDR Annex VIII then, this type of device should be considered under the “type of device” while consulting the expert panel.
Other examples for the same type of purposes include
Automated and semi-automated devices
Technologies
Multiplex and single analyte devices
Kits and class D components of those kits
Control materials
Hence, the notified body issuing the certificate should check if the product meets the criteria stated above to classify it as the “type of device” for the first time.
For the final decision, they can use their knowledge and expertise, consider the information provided by the manufacturer, or if the device has already undergone an expert panel consultation.
Post assessments, if the notified bodies decide that the product is given the first certification, they need to consult the expert panel and document the certification with the conclusion.
Fig 1: Notified body template for the expert consultation
If the expert panel has been kept in consultation for the first certification of the IVDR devices, the notified body cannot issue the second or third certificate without considering the views of the expert panel on the type of device.
What are class D IVDR devices?
Class D devices are high-risk devices, including devices used for blood screening for grouping, to screen cells & organs to manage infectious outbreaks or for transplantation.
What is an expert panel?
Expert panel advisors are appointed by the EU commission who can provide scientific, technical, and clinical evaluation guidance for high-risk devices and their performances.
Disclaimer: Regulations/legislations are subjected to changes from time to time and the author claims no responsibility for the accuracy of information.
Market surveillance is the activity carried out by the competent authorities according to Article 93 of MDR 2017/745 to ensure that products on the market comply with the relevant laws and regulations and with the current EU health and safety requirements. Maintaining market security in Europe and promoting consumer safety and business trust is vital.
Suppose the medical device poses an unacceptable risk to the health or safety of the patients, users, or other people or any other aspects of the protection of public health.
In that case, the competent authorities shall immediately require the manufacturer of the medical devices concerned, its authorized representative (AR), and all other relevant economic operators to take appropriate and duly justified corrective actions to bring the device into compliance with the MDR Regulation or withdraw or recall the medical device from the market.
Depending on the severity of the incident, the regulatory authorities require reports of serious adverse events or accidents to be submitted within 48 hours to 15 days.
The most crucial aspect of market surveillance efforts is the evaluation and examination of the adverse event or incidence investigation reports, risk management reports, and vigilance data from medical device manufacturers and consumers.
If they disagree with the national legislation notified, they must immediately communicate their complaints to the European Commission and the other Member States via the electronic system referred to in Article 100 of MDR.
Any measures taken by a Member State that has not been objected to by either a Member State or the Commission within two months of receiving the notification are justified.
If necessary, the authority may start a public field safety corrective action (FSCA). For significant product non-conformities, the responsible authority must evaluate if further regulatory action is necessary, which can be taken by destroying hazardous or non-compliant products, confiscating medical equipment, or assisting the manufacturer in bringing the product back into compliance with the law.
Obligations of the competent authorities are
Monitoring devices and incidents that occur while using them
Analyzing market data and identifying the possible potential issues
Reviewing technical documentation
Identifying unsafe or non-compliant medical devices
Reactively or proactively inspecting economic operator facilities
Removing unsafe devices from the market
The competent authorities shall develop annual surveillance activity plans and allocate adequate materials and qualified human resources to carry out those activities above.
Also, they shall prepare a summary of the surveillance activities performed with the required corrective action to be set out by the economic operators and make them available on the electronic system.
The Member States will review and evaluate the effectiveness of their market surveillance efforts, which are carried out at least every four years, and be informed to the Commission and other Member States of their outcomes.
Each Member State must summarise the results available to the public via the electronic system, as mentioned in Article 100 of MDR 2017/745.
The electronic system EUDAMED shall collate and process the following information on market surveillance.
Surveillance activity results
Final inspection report
Unacceptable risks associated with the medical devices
Non- compliance product information
Results of reviews and assessments carried out by the Member states on market surveillance.
To ensure a high-quality and uniform level of market surveillance across all Member States, the competent authorities must coordinate their market surveillance efforts through joint market surveillance activities, work together, and share their results with one another and the Commission.
What is the difference between Post-market Surveillance (PMS) and Market Surveillance?
Market surveillance is the same as post-market monitoring, where they make sure that medical devices sold on the EU market are safe, effective, and compliant. Market monitoring is conducted by the appropriate competent authorities, whereas the manufacturer of the medical devices carries out PMS.
What is the role of vigilance in market surveillance activities?
Vigilance focuses on reporting serious adverse events or accidents and field safety corrective actions (FSCA). In contrast, market surveillance is entirely concerned with developing procedures that can ensure the compliance of medical devices.
Any serious incident involving a device marketed and sold in the European Union and any field safety remedial action carried out in the EU or other markets where the device is sold should be made available in EUDAMED.
What is a joint action of market surveillance?
The Joint Action on Market Surveillance of Medical Devices (JAMS) is created to strengthen market surveillance across European member states. The medical device industry carries out best practices, education, information, and resources to improve public health protection. Critical goals include enhancing coordination and assisting member states with limited resources in building their capacities and skills in the market surveillance network. It will facilitate the creation of clinical processes, equivalent resources, and a consistent and balanced approach to manufacturer inspections.
Article 11 of the Regulation (EU) 2017/745 on medical devices (MDR) and EU Regulation (EU) 2017/746 on in vitro diagnostic medical devices (IVDR) outlines the obligations and responsibilities for the Authorised Representatives (AR).
Key points are taken for Authorised Representatives in accordance with the guidance:
A ‘sole’ authorised representative means a manufacturer can have more than one Authorised Representatives (AR) for different generic device groups. However, for one specific generic device group, the manufacturer should designate only one Authorised Representatives (AR).
On behalf of the manufacturer, Authorised Representatives (AR) can lodge an application for conformity assessment according to Annex IX, X, XI MDR/IVDR with a notified body at the pre-market stage.
AR who terminates the mandate may still cooperate with the competent authority for devices which was designated by them, particularly when no new AR has yet been designated for those devices.
AR must be registered under EUDAMED as per Section 1 of Part A of Annex VI of the Regulations, which needs to be updated within one week of any change occurring and the accuracy of the data at intervals no later than one year after the initial submission of the information, and every second year thereafter.
AR name shall appear on relevant documentation such as the EU DoC (Declaration of Conformity) and device labelling by the manufacturer.
The legal representative established by the sponsor of the clinical investigation or performance study is not defined under the AR requirements.
AR shall keep a copy of the technical documentation and the EU declaration of conformity for at least ten years after the last device covered by the EU DoC and 15 years for implantable devices.
‘Permanently available’ means it is mandatory for the manufacturer to provide the requisite documentation in their most recent versions and certificates. This includes amendments or supplements, either in hard or electronic copy to the AR. In practical terms having permanent access to such documents.
When the liability of the AR is alleged within the framework of a specific legal regime for defective products, the AR is afforded the same rights to defend itself as the manufacturer under that regime.
In the event of a problematic termination like non-compliance or non-traceability with the manufacturer, the out-going AR is also advised to inform the competent authorities and, where applicable, the notified body.
In general, a tripartite agreement should exist, except in cases where this is ‘not practicable’ to involve the outgoing AR, the obligation under Article 12(d) to forward complaints to the manufacturer or incoming AR should apply.
AR may be consulted for market surveillance measures taken by competent authorities to make documentation and information available to them. Also, AR may be subject to announced and unannounced inspections by the competent authorities as part of their market surveillance activities which is also covered for the legacy devices.
New guidelines on how to distinguish between medical devices and medical products under the Medical Devices Regulation have been published by a working group of the European Commission (MDR).
The new recommendations from the European Medical Device Coordination Group (MDCG) cover “borderline products” that are difficult to classify as either medical devices subject to the MDR requirements or medical products for human use subject to the requirements of Directive 2001/83/EC (MPD) for CE Marking.
The agreements reached by the Member State members of the Borderline and Classification Working Group (BCWG) following the exchanges under the Helsinki Procedure in accordance with Regulation (EU) 2017/745 on medical devices (the MDR) and Regulation (EU) 2017/746 on in vitro diagnostic medical devices are explained in the document, which will be referred to as the manual (the IVDR).
The specific document here explains the goals and workings of the Helsinki procedure. The BCWG is presided over by the European Commission and comprises observers from a number of stakeholder associations and representatives of all Member States’ relevant agencies.
The document outlines the methodology for classifying medical devices per the new regulatory framework. At the same time, the document itself is not legally binding and is not meant to establish new regulations or responsibilities. Instead, it further explains the relevant regulatory requirements and suggests considerations for ensuring compliance.
It is clearly emphasised that the current document is not intended to represent the EC’s official viewpoint. Additionally, should it be deemed reasonable to do so to reflect comparable adjustments to the underlying rules, the MDCG maintains the right to make changes to the document and suggestions included within.
Regulatory Background
As a general rule, it is the responsibility of the authorities of the Member States where a product is on the market to determine whether it qualifies as a medical device and to apply the classification requirements.
The MDCG also recognises that there may be variations in the methods used depending on how the applicable classification rules and regulations are interpreted. The MDCG believes it is crucial to create a widely followed protocol that will be adhered to by all parties engaged in activities involving medical devices in the EU.
The agreement that the Member States reached following their interactions under the MDR and IVDR of the Helsinki Procedure is described in the manual.
Scope
The manual defines borderline cases as situations where it is not immediately evident whether a particular product is a medical device, an in vitro diagnostic medical device (IVD), or neither.
Additionally, it is indicated that some of the requirements found in other articles of the Regulations, including those that list the products exempt from the Regulations’ purview, may also be applied.
However, in some circumstances, even if the product in question does not fit the definition of a medical device or is expressly exempt from regulation under the regulation, other EU-wide rules or national regulations may still apply.
These situations are not covered by the present manual, which only covers the aspects of using the qualification rules outlined in the Regulations.
The document also refers to the MDCG guidance on the distinction between medical devices and pharmaceuticals under the Medical Devices Regulation (EU) 2017/745, as well as the relevant guidance on the qualification and classification of software under Regulations (EU) 2017/745 and 2017/746.
The relevant regulations further state that after it is established that the product in question is a medical device, a risk-based classification should be carried out, resulting in the device being given the proper risk class (from I to III).
The risk classes to be used are A, B, C, and D if the product under consideration is a medical device for in vitro diagnosis. As was previously indicated, under some circumstances, it becomes challenging for the competent authorities of the Member State to apply the requirements for medical device classification uniformly.
The competent authority should make its choice on a case-by-case basis, considering the details of the product in issue, as the suggestions offered in the current handbook are not all-inclusive.
Key Principles
Borderline Between Medical Devices and Medicinal Products
The following are only a couple of the instances given by the MDCG:
A nasal spray containing COVID-19 antibody is intended to render the virus inactive. Before anything else, it’s critical to identify the primary mode of action or how the product fulfils its intended function.
In this scenario, the main goal of the spray is accomplished by antibodies attaching to the virus; as a result, the virus cannot replicate and infiltrate mucosal cells.
Furthermore, it is said that a product that meets the general definition of a medical device is one whose intended action cannot be accomplished through pharmacological, immunological, or metabolic methods.
Accordingly, based on this criterion, the product in question should be controlled as a medicinal product rather than a medical device.
Graphite crucible used to create pictures of the patient’s airways using Technetium-99m radionuclide (to prepare an aerosol). While a gamma camera is used to capture an image, such an aerosol should be inhaled.
Any medicinal preparation that, when ready for use, has one or more radionuclides (radioactive isotopes) incorporated for medicinal purposes are radiopharmaceutical, according to the appropriate regulations. A kit is any preparation that must be reconstituted or mixed with radionuclides in the finished radiopharmaceutical, often before administration.
Due to the product’s intended use and planned mode of operation, it does not fulfil the definition of a medical device in this specific instance and is, therefore not subject to regulation under the medical device framework.
Borderline Between Medical Devices and Biocides
The guideline also explains the crucial distinctions between medical devices and biocides, governed by Regulation (EU) 528/2012, which deals with issues pertaining to biocidal goods intended for marketing and use in the EU.
The authority also offers many instances to illustrate the methodology used when making such a conclusion. For instance, an antibacterial and antiviral concentration is described in the first example as a water-based treatment for textile materials.
In this situation, the treatment in question does not fulfil the definition of a medical device. It should not be regulated as one because it is designed to affect the features of other items rather than apply to specific patients.
Other Types of Products
The guidelines scope also includes topics pertaining to substances with human origin, cosmetics, food, and personal protective equipment. A rescue bag is the first product that is described. It transfers patients during rescue operations to ensure their care and safety.
Such a bag, in particular, comprises components meant to guarantee the patient’s mechanical protection while transported, including various transport mechanisms. The main goal of the rescue bag is to prevent the patient’s condition from worsening due to any environmental influences during the rescue.
According to the authority, the product should be classified as a medical device because its intended use conforms to the medical purpose of easing or compensating for an injury or handicap, as stated in Art. 2(1) of the MDR; nonetheless, according to Rule 1, the risk class should be MDR class I.
Another illustration in the manual explains the Plexiglas box for caregiver protection, which is meant to be utilised to lower the dangers associated with the infection that could be spread during procedures.
In this regard, the authority explains that a product should not be classified as a medical device if its only purpose is to protect a caregiver or healthcare professional by preventing exposure during a medical or surgical operation.
Further, since a medical gadget is supposed to be used to safeguard the patient, such a motive could not possibly be its intended use.
FAQs
What does the Helsinki Procedure mean?
The Helsinki Procedure is a procedure that “allows consultation among competent authorities (CAs) on borderline and classification issues concerning medical devices and to guarantee that relevant guidance is provided in the Manual on Borderline & Classification for Medical Devices.
Disclaimer: Regulations/legislations are subjected to changes from time to time and the author claims no responsibility for the accuracy of information.